Introduction
The Valsalva maneuver is a classical test for evaluating Eustachian tube function [1]. It involves patients forcefully exhaling to raise nasal air pressure while keeping their mouth and nostrils closed. This action passively opens the Eustachian tube, leading to bulging of the tympanic membrane as air pressure is transmitted into the middle ear. The mechanism is akin to that of the Politzer maneuver, though it relies on self-induced intranasal pressure increase [2]. In clinical practice, the Valsalva maneuver is recognized for its simplicity and convenience in evaluating the passive patency of the Eustachian tube. However, its effectiveness is limited by several drawbacks; notably, the variability in the pressure increase in the nasal cavity among individuals [3,4]. This inconsistency can result in false failure of the Valsalva maneuver.
An automated hand-held device, known as the middle ear inflation device (MEID), has been designed for politzerization, particularly benefiting children who frequently suffer from recurrent otitis media. Developed by Arick and Silman [5], the MEID delivers a regulated flow of air into the nasal cavity. Patients are instructed to close one nostril and their mouth, place the MEID in the open nostril, and activate it for 3 seconds. Following this, patients are asked to swallow to open the Eustachian tube.
While the MEIDвҖҷs primary objective is to alleviate symptoms associated with obstructive Eustachian tube dysfunction, including recurrent otitis media and tympanic membrane retraction, it also facilitates the assessment of the Eustachian tubeвҖҷs patency. Unlike the Valsalva maneuver, the MEID provides airflow at a relatively consistent pressure within the nasal cavity. Consequently, we have introduced the вҖңPopper test,вҖқ wherein a positive result indicates bulging of the tympanic membrane upon using the MEID, and a negative result indicates an absence of bulging. This study aimed to validate the effectiveness of the Popper test as compared to the traditional Valsalva test within the same individual, proposing that the controlled air supply offered by the MEID makes the Popper test a viable alternative.
Subjects and Methods
Study enrollment
Between June 1, 2023, and August 1, 2023, new patients visiting the corresponding authorвҖҷs clinic were routinely subjected to both the Valsalva test and the Popper test, provided their tympanic membranes appeared normal. Out of the 144 ears assessed, 64 were excluded based on the following criteria: 1) a history of ear surgery; 2) the presence of a patulous Eustachian tube; 3) tympanometry type B; and 4) indeterminate middle ear pressure. Consequently, the study included 68 ears with tympanometry type A and 12 with tympanometry type C. The Institutional Review Board (IRB) of our center approved this study (project number: 3-2024-0029), which adhered to the principles of the Declaration of Helsinki. Due to the studyвҖҷs retrospective nature, the requirement for informed consent was waived by the IRB of Gangnam Severance Hospital.
Test protocols
For the Valsalva test, patients were instructed to inflate their cheeks and nasal cavity by forcefully exhaling with their mouth closed and nostrils pinched. After practicing several times, patients were asked if they understood how to perform the Valsalva test. Those who indicated they did not understand were placed in the вҖңunableвҖқ group. For those who understood, the inflation of their tympanic membranes was observed using otoendoscopy as they performed the Valsalva test.
Subsequently, the Popper test was conducted using the MEID (Eustacure; Mega Medical, Seoul, Korea). Patients were instructed to block the contralateral nostril with their finger, keep their mouth closed, and hold their breath. The MEID was then applied to the unblocked nostril for 3 seconds, after which patients were asked to swallow. The inflation of the tympanic membranes was observed with otoendoscopy during the swallowing action.
Result
A total of 68 ears from 40 participants were classified as having normal middle ear pressure (Table 1). The average age of the participants was 48 years, and the mean middle ear pressure was -12.4 daPa. Among these, 30.9% were unable to perform (unable group) the Valsalva maneuver despite receiving instructions. Thirty-one participants (45.6%) successfully inflated their tympanic membrane (success group) by performing the Valsalva maneuver. Conversely, the MEID successfully inflated the tympanic membrane in 88.2% of the cases.
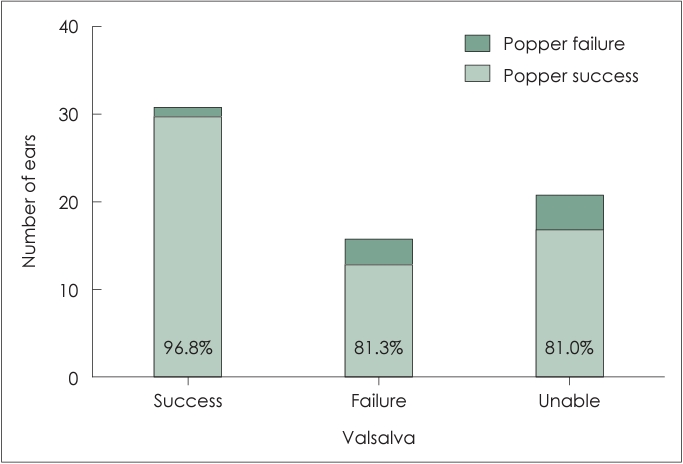
Within the group that succeeded in the Valsalva maneuver, 96.8% also managed to inflate their tympanic membrane using the MEID (Fig. 1). Among those who failed or were unable to perform the Valsalva maneuver, 81.3% and 81.0%, respectively, succeeded in inflating their tympanic membrane with the MEID. Further, we assessed the sensitivity and specificity of the tests among individuals with negative middle ear pressure, defined as a middle ear pressure <-100 daPa (Table 2). Excluding the Unable group those who unable to perform the Valsalva maneuver, the sensitivity and specificity of the Valsalva maneuver were 50% and 66% respectively. In contrast, the Popper test demonstrated a sensitivity of 25% and a specificity of 88%.
During the Valsalva maneuver and the Popper test, there were no complications (ex: otalgia, epistaxis, fainting etc.).
Discussion
The findings of this study revealed that the Popper test has higher specificity but lower sensitivity compared to the Valsalva test. Additionally, approximately 31% of participants were unable to perform the Valsalva maneuver despite receiving instructions. Within the group that succeeded in the Valsalva test, 96.8% also showed a positive outcome in the Popper test. For those who either failed the Valsalva test or were unable to perform it, the Popper test yielded positive results in 81.3% and 81.0% of cases, respectively.
Previous research has shown that the objective Valsalva test, where the tympanic membrane is examined through endoscopy or impedance audiometry, produces positive results in 51.7% to 88.8% of healthy individuals [6-9]. In our study, only about 66% of individuals with normal middle ear pressure had a positive result from the Valsalva test. This variance suggests that the outcomes of the Valsalva test can significantly depend on either the individual or the instructorвҖҷs technique. Intriguingly, the success rate for the Popper test stood at 88.2%, which is similar to highest success rate of the Valsalva test reported in prior studies [6]. Moreover, the success rates of the Popper test were comparable between those who failed the Valsalva test and those unable to perform it, at 81.3% and 81.0%, respectively. This may be because the Valsalva failure group might not actually be unable to open Eustachian tube; rather, they might be more similar to the group unable to perform the Valsalva maneuver.
To our knowledge, there is a scarcity of reports on the proportion of individuals who are unable (as opposed to failing) to perform the Valsalva maneuver to inflate the tympanic membrane. Previous studies have noted that a failure in the Valsalva maneuver does not necessarily imply Eustachian tube dysfunction [10,11]. In this study, 30.9% of participants were classified in the вҖңunableвҖқ category for the Valsalva test. It may be because we defined the вҖңunable groupвҖқ as those who expressed uncertainty about the procedure after receiving initial instructions. Furthermore, the Valsalva testвҖҷs relatively low success rate (66%) may be attributed to inadequate instruction on how to properly execute the maneuver. It suggests that performing the Valsalva maneuver effectively might require more comprehensive training and practice.
The Popper test, benefiting from the controlled airflow supplied by the MEID, proved more reliable than the Valsalva test, with none of the patients categorized as вҖңunable.вҖқ However, the diagnostic performance of the Popper test can be significantly affected by the MEIDвҖҷs characteristics. For instance, a study by Hidir, et al. found that using a different MEID model (EarPopper, EP-3000; Micromedics, Inc., St. Paul, MN, USA) was effective in only 43.3% of cases. The MEID utilized in our research (Eustacure) delivers air pressure levels of 4.5-5.5 psi, which exceed those provided by the EarPopper [5]. Accordingly, our study observed a higher success rate (88.2%); however, the sensitivity might be reduced due to the higher air pressure generated by the MEID. In addition, the low sensitivity may result from the poor diagnostic value of the tympanometry test for diagnosing Eustachian tube dysfunction [12]. Notably, 75% of tympanometry type C cases (middle ear pressure <-100 daPa) demonstrated a positive outcome in the Popper test.
Since balloon Eustachian tuboplasty (BET) was introduced, the Valsalva maneuver has been used not only as a surgical indication but also as a measure of surgical outcomes [13-15]. This implies that a false failure of the Valsalva maneuver, corresponding to the вҖңunableвҖқ group in this study, can lead to the failure of BET. In addition, reducing the false failure of the Valsalva maneuver is crucial to prevent BET in contraindicated patients. The clinical importance of the Popper test, as suggested in this study, is to minimize the ambiguity of the Valsalva maneuver and reducing the false failure rate. Although the sensitivity of the Popper test in this study was very low, its higher specificity (88%) suggests that the Popper test is a promising alternative to the Valsalva maneuver for preventing unnecessary BET.
This study had a limitation. While we consecutively enrolled patients visiting the clinic and used tympanometry to exclude potential Eustachian tube dysfunction, the individuals enrolled were not healthy controls. Also, considering the failure rate of the Valsalva maneuver, which is approximately 31%, there is a possibility that the patients did not fully understand and perform it correctly. In addition, the retrospective cross-sectional design of the study and the small number of enrolled patients are additional limitations. In the future study to develop this reserch, the result of the Popper test should be validated according to the disease entity.
In conclusion, the MEID may serve as an alternative to the Valsalva test, potentially enhancing reliability by accounting for individual variations in performing the Valsalva test. However, it is possible that the diagnostic performance of the MEID significantly depends on its specific properties.