Introduction
Grisel’s syndrome is defined as subluxation of the atlantoaxial joint, unrelated to trauma or bone disease. Atlantoaxial subluxation is observed after head and neck infection, such as tonsillitis, pharyngitis, cervical abscess, and otitis media [1,2]. Moreover, it is an uncommon complication of otolaryngological procedures, including tonsillectomy, adenoidectomy, pharyngoplasty, mastoidectomy, and tympanoplasty, which most commonly develops in the pediatric population [1-3]. Only seven cases of Grisel’s syndrome have been reported in South Korea [4-10]. Four cases were noted in children. Two patients had acute lymphadenitis, and the other two had upper respiratory infection. One adult case following tonsillectomy in a patient with tonsillar cancer with preoperative radiotherapy was reported [9]. Five cases following tonsillectomy and adenoidectomy have been reported worldwide [11]. Only one case after adenotonsillectomy was reported in South Korea [10].
This report presents a case of Grisel’s syndrome in an 8-year-old girl who presented with neck pain and torticollis after tonsillectomy and adenoidectomy.
Case
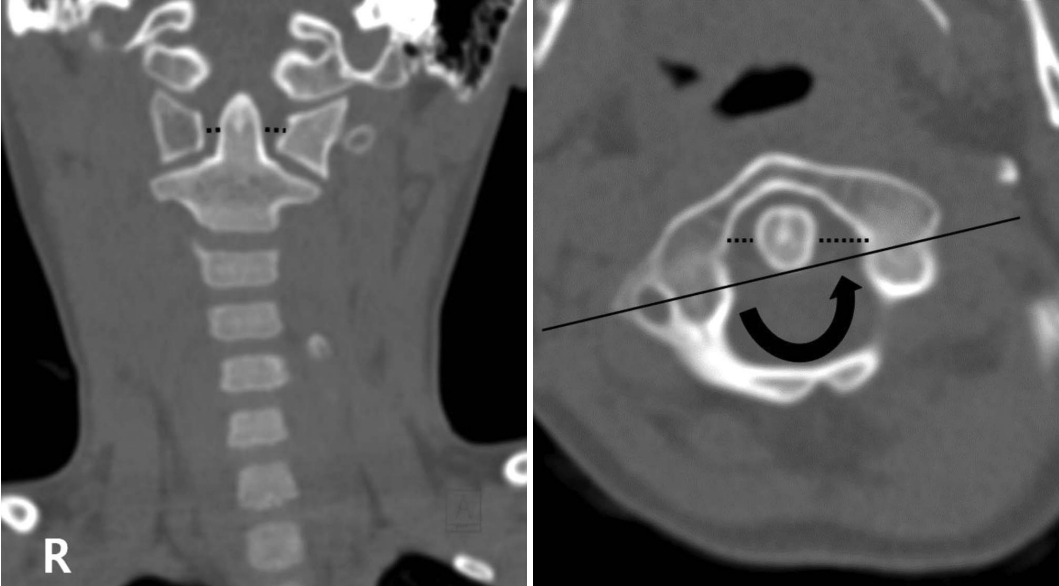
An 8-year-old Korean girl was referred for evaluation of snoring and sleep apnea. She had grade 3 tonsillar hypertrophy and adenoid vegetation in the physical examination and paranasal sinus view radiography. In August 2020, she underwent tonsillectomy and adenoidectomy. The tonsil was removed with monopolar bovie, and bipolar cautery was used for hemostasis. Endoscopic debrider adenoidectomy and monopolar suction cauterization were performed. The patient was discharged on the day after surgery without any complications. On postoperative day 5, she visited our outpatient clinic due to neck pain and torticollis. Neurological examination results were normal. Radiological evaluation, including radiography of the cervical spine with anteroposterior, lateral, and open mouth view, and CT and MRI were done. In radiography, atlantoaxial rotatory subluxation was suspected (Fig. 1). CT and MRI showed Type 1 atlantoaxial rotatory subluxation (Fig. 2) with mild prevertebral soft tissue edema. The anterior atlantodental interval was 2.4 mm, which was normal. Asymmetric widening of the gap between the left lateral mass of atlas and odontoid process was noted with narrowing of gap between the right lateral mass of atlas and odontoid process (Fig. 2). There was no visible acute fracture or significant abnormality in both sternocleidomastoid muscles. The patient was diagnosed with post-tonsillectomy and adenoidectomy Grisel’s syndrome.
She was immediately hospitalized in the pediatric orthopedics department for reduction. She was placed in 2-kg cervical halter traction for approximately 5 days. She also received conservative treatment with appropriate oral antibiotics and analgesics. The following day after reduction, repeat radiography showed complete reduction of previous atlantoaxial rotatory subluxation (Fig. 3). The patient received three more days of halter traction after complete reduction and was then discharged from the hospital.
Radiography was performed 7 days after discharge. It showed no abnormalities. After 6 months of follow-up, she had completely recovered without recurrence of subluxation.
Discussion
Grisel’s syndrome mainly develops in the pediatric population. Approximately 90% patients with Grisel’s syndrome are <21 years old [12]. The pathogenesis of Grisel’s syndrome is unusual and poorly understood [1,2]. The atlantoaxial joint stability is mostly attained by two ligaments. The transverse ligament is the primary stabilizer of the atlantoaxial joint. It supports the posterior odontoid process and prevents excessive shift of the atlas to the axis. The alar ligaments are secondary stabilizers that prevent pathological rotation [12].
The first hypothesis is that pre-existing laxity of the above mentioned ligament and instability of the atlantoaxial joint lead to non-traumatic atlantoaxial subluxation [12,13]. Some morphological and functional differences are found in children, such as larger head size; weaker cervical muscles, looser ligament, and joints; and shallower and more horizontally placed facet joints [2]. These characteristics are more likely to cause instability of the atlantoaxial joint in children than in adults. Moreover, Down’s syndrome is a common example of this disease related to ligamentous laxity, which results in high risk of atlantoaxial subluxation. Neck extension is required in many head and neck surgeries, including tonsillectomy and adenoidectomy, and leads to instability of the atlantoaxial joint.
The second hypothesis is that parapharyngeal septic effusion (may arise from the operative field or other sources in the upper airways or head and neck infection) was transported to the periodontal venous plexus via the pharyngovertebral veins [1,3]. Hematogenous spread to the cervical spine leads to hyperemia and results in cervical spine decalcification and weakening of the ligaments, followed by excessive rotation of C1 on C2. Moreover, bipolar or monopolar cauterization may result in thermal injury to the adenoid or tonsil bed tissue and contributes to wound infection, which can lead to atlantoaxial subluxation as previously described [14].
Battiata and Pazos [13] had proposed a “two-hit” hypothesis about the pathogenesis of Grisel’s syndrome. The first “hit” is pre-existing cervical ligamentous laxity. The second “hit” is a subsequent local infectious process, weakening the pre-existing loose ligaments, and eventually leading to atlantoaxial subluxation.
In our case, we hypothesize that neck extension led to instability of the ligaments and local infection following monopolar cauterization on the adenoid tissue, which acted as a “hit.”
Grisel’s syndrome mainly presents with neck pain, head tilt, and neck restriction after head and neck infection or after otolaryngological procedures. Acute painful torticollis is typically the first symptom in many cases of Grisel’s syndrome, including our case [1-3]. Another patient may also present fever with nonspecific signs of infection [4]. In a few cases, neurological complications from mild paresthesia to quadriplegia were also observed and can lead to acute respiratory failure and finally death [4,5].
Physical examination is important. When our patient visited the outpatient department, she had acute painful torticollis. We initially suspected a retropharyngeal abscess. However, there is no evidence of retropharyngeal abscess on lateral neck radiography. Thus, we searched similar cases of acute painful torticollis and finally found some cases of Grisel’s syndrome following tonsillectomy and adenoidectomy. Then, we immediately performed CT and MRI for diagnosis and provided early and successful treatment.
The key step in diagnosis is suspicion of Grisel’s syndrome. Patients who have acute neck pain and torticollis with Down syndrome or with history of otolaryngological procedures or infection should suspect this syndrome [1,2]. In case of suspicion, radiography such as plain radiographs, CT, and MRI are performed to confirm the diagnosis.
Plain radiographs of the cervical spine may show asymmetry between the lateral mass of C1 and odontoid process in the anteroposterior view and increased atlantodental interval in the lateral view [1]. CT can be helpful to detect the bony cervical spine, and MRI is useful to find abnormalities in the surrounding soft tissue structures and the spinal cord. CT is the most useful diagnostic tool regarded as the golden standard [1,3].
Fielding, et al. [15] classification of C1-C2 rotary subluxation is differentiated by the degree and direction of atlas displacement.
In type I, C1 is rotated on C2 with anterior displacement of less than 3 mm. In type II, C1 is rotated on one articular process of C2 with 3-5 mm anterior displacement. In type III, C1 is rotated on both articular processes of C2 with anterior displacement of greater than 5 mm. type IV is indicated by rotatory fixation with posterior displacement of the atlas. Type I and II subluxations generally have no neurological symptom. However, type III and IV can have neurological complication related to spinal cord damage. MRI of our patient showed normal atlantodental interval of approximately 2.4 mm (type I subluxation).
We cannot change the surgical method because Grisel’s syndrome is unpredictable. However, in our opinion, it is better to avoid excessive neck extension as much as possible to prevent ligament instability. In addition, since excessive monopolar cauterization to control bleeding after adenoidectomy can act as a risk factor for Grisel’s syndrome, local epinephrine injection before the procedure and epinephrine cotton ball packing immediately after the procedure can help control bleeding and then reduce the use of monopolar cauterization. Although these preventive measures can be used, they are unlikely to be practical because Grisel’s syndrome’s incidence is very low. So, it is important to suspect Grisel’s syndrome based on patient’s symptoms, physical examination, and radiologic finding because Grisel’s syndrome may be fatal with delayed diagnosis.
However, early diagnosis can lead to a better prognosis in terms of neurologic complications associated with spinal cord or radicular compression [2]. Once the diagnosis is clear, treatment should be initiated urgently. Traditionally, type I and II without neurologic symptoms may be treated with antibiotics and cervical collars. However, some patients who do not respond to conservative treatment need cervical traction, and subsequently need to apply neck immobilizers like cervical collars or halo vest about 6 weeks to prevent recurrence of the subluxation [1]. Type III and IV need more aggressive treatment, such as bed rest with cervical traction, and subsequently need to apply neck immobilizer. Any patient who has neurologic symptoms or fails to achieve reduction should undergo immediate arthrodesis of the first and second cervical vertebrae [1-3]. In some cases including our case, active treatment (such as cervical traction) in the early stage (Feilding type I and II) results in good prognosis [2,4,7].
In conclusion, Grisel’s syndrome is an extremely rare and poorly understood. However, it leads to life-threatening complications, such as quadriplegia, when it is diagnosed late. Thus, every ENT doctor suspects this syndrome in children who have acute torticollis with or without neck pain following head and neck surgery or infection. In our opinion, it is better to avoid excessive neck extension and monopolar cauterization. Early diagnosis and treatment prevent catastrophic outcomes and lead to good prognosis.