Introduction
Chronic otitis media (COM) is a common disease, its incidence has been reported as 2% of the worldwide population [1]. Following the data from the Korean National Health and Nutrition Examination Survey 2010-2012, Korean prevalence of COM was 3.8%, which is slightly higher than the average of worldwide [2]. There has been many treatment ways including medication, frequent dressing and surgery to treat COM, but surgery still remains a key treatment of COM and COM related complications [3,4].
Decisions about whether or not to perform ear surgery of COM are made by an otolaryngologist based on various clinical results [5]. Patients with COM were performed many clinical evaluation such as physical examination, pure tone audiometry (PTA), temporal bone computed tomography (TBCT) before surgery. However, many of otolaryngologists are likely to overlook how much suffering a patient has due to COM. Also, as there were insufficient tools to quantify the patientÔÇÖs discomfort due to symptoms of COM, the severity of the patientÔÇÖs symptoms and the impact on the quality of life were dependent only on the patientÔÇÖs each level of expression [6].
The Health-Related Quality of Life (HRQoL) which means the degree of patientÔÇÖs satisfaction of their life influenced by disease, and it concerns patientÔÇÖs total health status [7]. In the assessment of healthcare, patient-based measuring instruments regarding the quality of life and perceived handicap have become increasingly important [8]. To develop measurement of disease-specific HRQoL of COM, Phillips, et al. [8] developed the Chronic Otitis Media Questionnaire-12 (COMQ-12) using selected questions from following tools; chronic ear survey (CES), Chronic Otitis Media Outcome Test-15 (COMOT-15), COM-5 [1,8-10].
The original version of COMQ-12 was made in English, and needed to develop other language version to use the COMQ-12 widely so that many of COM patients would benefit. Dutch, Russian, Portuguese, Servian, as well as Indian Kannada version are already validated, but no other language version is used yet [11-16].
In our study, we assessed the validity of Korean version of COMQ-12 (K-COMQ-12) and correlation with the disease activity of COM classified according to physical examination. Also we found meaningful cut-off values between COM patients and normal subjects using K-COMQ-12.
Materials and Method
The original authorÔÇÖs agreement
The corresponding author sent e-mail to Dr. John Phillip, the original author of COMQ-12, and obtained permission and received the original version of COMQ-12.
The K-COMQ-12
The original English version of COMQ-12 consists of 12 questions. Each item is scored from 0 to 5, the higher number the more discomfort it means. The original COMQ-12 was translated from English to Korean by bilingual otolaryngologist in English and Korean. Next, the translation was checked by a person who majored in Korean literature. Then the naive Korean version was translated back to English. Both the original and retranslated English version of the COMQ-12 were compared by a person who majored in English literature and suggested minor changes (Appendix 1).
Subjects
Power analysis were performed to estimate the number of subjects (effect size 0.28, a-risk 0.05). In total, 212 individuals were enrolled in this study. One hundred and six patients who visited Yonsei University Wonju Severance Christian Hospital and diagnosed COM and planned surgery were enrolled in the study. To compare with control group, 106 healthy volunteers who have not experienced COM were asked randomly from Yonsei University Wonju Severance Christian Hospital.
All subjects participated in informed voluntary consent, and were independently answered each question of K-COMQ-12. In case of COM patients, they answered to K-COMQ-12 before they took surgery. There was no reported difficulties answering each question, and participants received no help in answering questions. Patients who could not read and understand the Korean-language were not enrolled in this study. Demographic informations of subjects such as patientÔÇÖs sex, age and body mass index (BMI) were collected. Informations of medical history, including hypertension, diabetes mellitus, lung or heart disease, cerebrovascular accident, chronic kidney disease, liver disease and frequency of noise exposure were also collected.
The Institutional Review Board of Yonsei University Wonju Severance Christian Hospital approved this study (CR316063).
Statistical analysis
Statistical analysis was conducted using the Statistical Package for Social Sciences Software (SPSS 22.0 IBM Corp., Armonk, NY, USA). CronbachÔÇÖs alpha and item-total correlation were measured to evaluate internal consistency. We used Kaiser-Meyer-Olkin (KMO) test to measure sampling adequacy. KMO value is considered ÔÇśgoodÔÇÖ if it is greater than 0.70, and ÔÇśexcellentÔÇÖ if it is greater than 0.90. Generally, it is known that factor analysis is appropriate if the KMO value is greater than 0.7. We also performed factor analysis, and the number of factors was determined using the eigenvalue and scree plot curve. Varimax rotation was used to simplify the interpretation of data. The independent t-test and one-way analysis of variance with Bonferroni method for continuous variables, chi-square or FisherÔÇÖs exact test for categorical variables were performed to construct validity. To facilitate the clinical interpretation of K-COMQ-12 scores, a threshold score for distinguishing normal from patients of COM was derived from the receiver operating characteristic (ROC) curve. We assessed significant differences when the p-value was less than 0.05 (p´╝ť0.05).
Results
Reliability
For the K-COMQ-12, CronbachÔÇÖs alpha was 0.939, suggesting good internal consistency. We also assessed item-total correlation coefficients. It ranged from 0.548 to 0.822 that indicates all individual items correlated well with the total score (Table 1).
Factor analysis
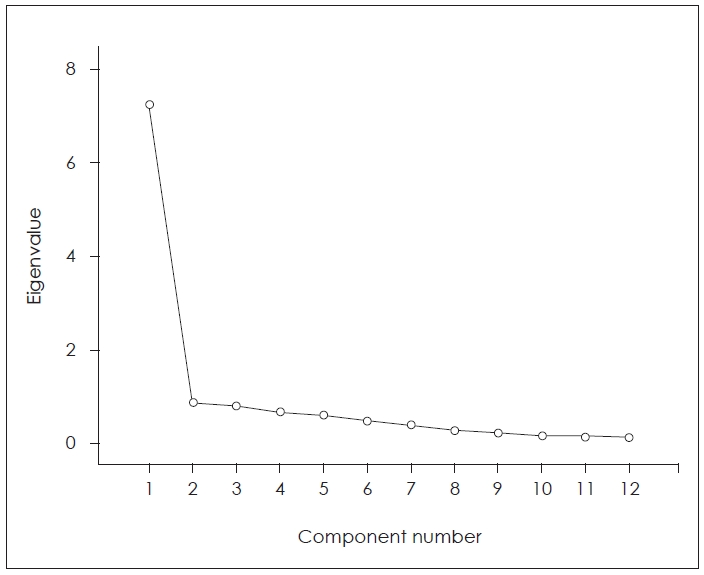
As the KMO value was 0.884, factor analysis is appropriate for our data. Factor analysis is generally used to group items of questionnaire with similar features. We determined the 2 factors were extracted using eigenvalues and a scree plot curve (Fig. 1). They explained 60.26% and 7.33% of all items of K-COMQ-12. The factor 1 includes 9 items (item 3, 4, 5, 6, 7, 8, 10, 11, 12), and the factor 2 includes 3 items (item 1, 2, 9) (Table 2). However, we could not find appropriate titles covering the items that make up each factor.
The item-communality values, which refers to the amount of variance of an item as predicted by the loading factor, ranged from 0.451 to 0.787 (Table 3). Generally, it is considered that each item loads well on factor when the value of communality is greater than 0.45.
Construct validity
We assessed the construct validity of K-COMQ-12 by comparing scores from COM patients to those of the control group. Among total 212 subjects which consist of 106 COM group and 106 normal group, clinical baseline characteristics of each group are shown in Table 4. There were no significant differences in many factors including subjectÔÇÖs age, sex, BMI and their medical histories. 34.9% of COM patients were performed previous ear surgery, 14.2% of COM patients had experience of noise exposure, and 11.3% had or had been wearing hearing aids in the past. They were statistically significant when comparing normal group (Table 4).
The control group showed 1.99 of mean K-COMQ-12 score [4.34 of standard deviation (SD)] whereas the COM group showed 22.69 (12.41 of SD), and they were statistically significant (Table 5).
Disease activity of COM and K-COMQ-12 scores
We classified the severity of COM according to the surgery which the patient decided to undergo. Typically, long-lasted infection with poor Eustachian tube function induces relatively severe COM, and usually requires mastoidectomy, however, tympanoplasty only is often sufficient for COM with relatively intact eustachian tube function and relatively short-lasting COM [17]. Following the type of surgery, 106 COM subjects were divided into two groups; the ÔÇśTympanoplasty onlyÔÇÖ group and the ÔÇśMastoidectomyÔÇÖ group. The ÔÇśTympanoplasty onlyÔÇÖ group was defined as COM patients who underwent only tympanoplasty without mastoidectomy after an evaluation by otolaryngologist, and ÔÇśMastoidecotmyÔÇÖ group was defined as COM patients who decided to undergo mastoidectomy regardless of whether tympanoplasty was performed or not. Among 106 of COM subjects, 38 were tympanoplasty only group and 68 were mastoidectomy group. The score of K-COMQ-12 showed significant differences among control, ÔÇśTympanoplasty onlyÔÇÖ group and ÔÇśMastoidectomyÔÇÖ group (p´╝ť0.001). However, in the post-hoc test, the difference in the K-COMQ-12 score between the ÔÇśTympanoplasty onlyÔÇÖ group and the ÔÇśMastoidectoy groupÔÇÖ was not statistically significant (p=0.700).
We tried to classify the COM subjects by the disease activity of COM according to the physical examination. ÔÇśInactive COMÔÇÖ group was defined as having no evidence of active infection with dried up tympanic membrane (TM) whether the perforation is or not on physical examination. ÔÇśActive COMÔÇÖ group was defined as showing wet TM or retracted or adhered TM to middle ear space. We also compared the score of K-COMQ-12 among the control, ÔÇśInctive COMÔÇÖ, and ÔÇśActive COMÔÇÖ group. The difference of K-COMQ-12 score according to the disease activity of COM based on physical examination were statistically significant among all three groups (p´╝ť0.001). The disease activity of COM goes higher, the K-COMQ-12 score went higher (Table 6).
Cut-off value of COM using K-COMQ-12
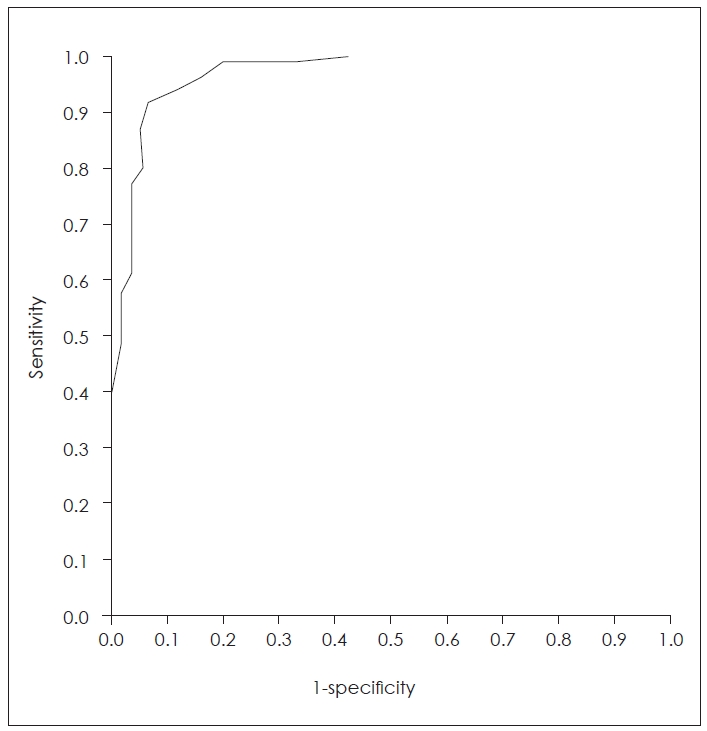
To assess the meaningful cut-off value between COM patients and normal group, the ROC curve was used (Fig. 2). The value of area under the curve was 0.969, which implies very high discriminatory power to distinguish subjects with the control and COM patients (p´╝ť0.001). We could also identify which cut-off point that indicates best balance between sensitivity and specificity using ROC curve. A cut-off score of 6 of K-COMQ-12 sets 0.915 of sensitivity and 0.934 of specificity. Therefore, using the K-COMQ-12 score of 6 of threshold, 91.5% of patients were correctly classified as COM, and 93.4% of non-patients were correctly categorized as normal.
Discussion
The patients-base measuring instruments of the HRQoL has become very important in healthcare. The COMQ-12 could provide information about symptoms they feel that are most important to the patients [8]. It allows clinicians to quantify the severity of the symptoms that COM patients feel. Even if the severity of the disease is similar with the clinicianÔÇÖs evaluation, it might be different in the inconvenience of each individual patient. Using COMQ-12, the clinician could identify the degree of discomfort caused by COM of the individual patient and determine how much the discomfort can be relieved during the treatment courses [8]. We translated COMQ-12 into Korean and tested it for validity, which allows patients with otitis media using Korean to use the tools to quantify the severity of their symptoms.
In our study, CronbachÔÇÖs alpha of K-COMQ-12 was 0.939, suggesting good internal consistency. It is the highest value than any other version of COMQ-12. The original version of COMQ-12 reported 0.889 of CronbachÔÇÖ alpha, Dutch, Russian, Portuguese, Serbian and Kannada version of COMQ-12 showed 0.833, 0.860, 0.85, 0.84, and 0.88 of CronbachÔÇÖs alpha value [8,11,13-16]. The item-total correlation coefficients of K-COMQ-12 ranged from 0.548 to 0.822. This indicates that all individual items correlated well with the total score.
Factor analysis was used to assess the internal structure of the K-COMQ-12, and two factors were identified according to eigenvalues and scree plot. However, there were no titles covering the items that make up each factor. Table 2 shows that items 5, 6, 9, 10, and 11 tend to be difficult to be classified as an specific factor. With the exception of these questions, the factor 1 can be defined as ÔÇťsymptoms associated with otorrheaÔÇŁ and the factor 2 as ÔÇťdiscomfort associated with hearing ability and tinnitus (hearing symptoms).ÔÇŁ However, this is not the preferred method. Besides, in original COMQ-12, eight questions (numbers 1-7 and 12) include severity of disease, whereas the remaining four questions (numbers 8-11) describe the frequency of disease occurrence, but they were not developed through factor analysis [8].
Our study shows that the K-COMQ-12 score in patents with a COM was significantly higher than that of the control group. The mean value and SD of K-COMQ-12 score showed 1.99┬▒4.34 in control group and 22.69┬▒12.41 in COM group. It was similar with the original version of the COMQ-12, and the follow-up study of normal patients [8,18].
After we divided COM group into subgroups according to the surgery the patient underwent which reflect the severity of COM, the K-COMQ-12 score goes higher as the severity of COM increased. However post-hoc test revealed there was no statistically significance between ÔÇśTympanoplasty onlyÔÇÖ group and ÔÇśMastoidectomyÔÇÖ group. As the authors of original version of COMQ-12 and the Russian, Portuguese, and Serbian versions were grouped by COM patients based on physical examination, compared the COMQ-12 scores, we also tried to divide COM patients following disease activity based on physical examination [8,13-15]. Considering that COMQ-12 is a questionnaire measuring inconvenience caused by COM, it is more appropriate to classify the patient based on the physical examination that reflects the disease activity. The score of K-COMQ-12 showed an increase as disease activity increased which is similar to the COMQ-12 validation study in other languages [8,13-15]. Therefore, The K-COMQ-12 score could be used an objective measurement tool reflects not only the difference between control and COM group, but also the disease activity of COM.
Our study shows that a cut-off value of 6 was determined between COM group and normal group. However, it is difficult to interpret K-COMQ-12 as a diagnostic tool. COM could be diagnosed only by simple consultation without the great effort of the clinician. Many of clinical results, including physical examination, PTA, TBCT could help to evaluation of COM, but not just based on this questionnaire. K-COMQ-12 is a tool that only reflects the patientÔÇÖs HRQoL of COM. As reported by Phillips, et al. [18], patients who reported lower score than the cut-off value of 6 in K-COMQ-12, are seriously considered before contemplating intervention [15].
Unusually, COM patients answered that they were more exposed to the noise than the normal group. They were aware that their impaired hearing ability due to COM makes listen to loud sounds in daily life. We thought that it is the result of relatively high noise exposure in COM patients.
In conclusion, the K-COMQ-12 is a reliable and valid tool to assess HRQoL in patient with COM. It has high internal consistency and the K-COMQ-12 could be also used as an objective tool that reflects the disease activity of COM. The cut-off value of 6 in K-COMQ-12 should be interpreted that having just statistical meaningful value, because of diagnosis of COM should be conducted by clinician based on various clinical results.